 The traditional surgical method for treating spinal stenosis in the past has been a fusion procedure using pedicle screws with relation to the lumbar (low back) spine. This procedure involves removing the disc (soft cushion between big bones in spine) and replacing it with a cage and bone graft material. Then, screws ultimately secure the level above the disc and level below the disc allowing those two vertebra (large bones in spine) to fuse. In summary, a fusion turns two bones into one.
The traditional surgical method for treating spinal stenosis in the past has been a fusion procedure using pedicle screws with relation to the lumbar (low back) spine. This procedure involves removing the disc (soft cushion between big bones in spine) and replacing it with a cage and bone graft material. Then, screws ultimately secure the level above the disc and level below the disc allowing those two vertebra (large bones in spine) to fuse. In summary, a fusion turns two bones into one.
This procedure has been done for decades and is very effective, but it does come with a cost. When you lose the motion of those bones due to fusion, the motion must be picked up elsewhere and this places increased stress on the adjacent levels. This often leads to increased re-operation rates. Because of this reason, spine research and innovation has shifted towards motion preservation techniques. Thus, the goal is two treat the pathology without sacrificing the loss of motion.
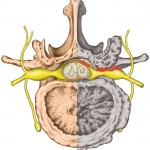
One massive game changer to the spine world has been the invention of intra-laminar devices such as the “Coflex”. The Coflex device is a simple titanium “U” shaped device that fits between the spinous processes, and has wings that fit around the superior and inferior spinous process. During this procedure, decompression is achieved, meaning that the spinal nerves and spinal cord are relieved of anything pressing on them. This is the goal of a spinal stenosis procedure, whether fusion or using the Coflex device. The fusion operation achieves this goal, but loses the motion that was previously there.
The beauty of the coflex device is that the motion is preserved. It is a very simple product that has excellent results. In the next few lines, we will explain the results of an FDA approved level one study of a fusion operation versus a coflex operation.
Here are the main points:
- Coflex saved an average of $5000-$8700 per case when compared to pedicle screw fusion for spinal stenosis.
- Coflex patients spent 40% less time in hospital compared to fusions patients.
- Coflex surgeries were 36% faster than fusion operations.
- Motion was preserved which was checked at 2 years post-op and which every patient maintained the same range of motion compared to pre-op. In the fusion operation, motion was lost.
- Coflex patients maintained normal adjacent level range of motion. Fusion patients did not. This is a tell tale sign that we often see with degeneration of discs. The first sign of degeneration is increased range of motion at adjacent levels.
- Average blood loss in fusion patients was 238.9 cc greater than in coflex procedures.
- Lastly and probably most importantly, coflex patients reported better outcomes at every time period including 6 weeks, 3 months, 6 months, 12 months, 18 months, and 24 months.
In summary, the coflex device is a game changer in spine surgery. Dr. Reginald Davis (the original study principal investigator) said it best,
“This is the first time a new spinal technology is proven better and more effective than the historical gold standard and is still actually lower cost.”
 At Prairie Spine & Pain Institute, we are thrilled to provide the coflex device for our patients . We were the first practice to use the Coflex device in the state of Illinois. We are able to perform a minimally invasive procedure, preserve the motion, and avoid the unnecessary fusion procedure. The coflex device is more affordable compared to fusion due to shorter operating time, faster patient recoveries, less blood loss, less narcotic usage, and shorter hospital stays, all with more sustained clinical success. If you’re suffering from spinal stenosis and considering surgery, come see us at Prairie Spine where the best options are made available to you.
At Prairie Spine & Pain Institute, we are thrilled to provide the coflex device for our patients . We were the first practice to use the Coflex device in the state of Illinois. We are able to perform a minimally invasive procedure, preserve the motion, and avoid the unnecessary fusion procedure. The coflex device is more affordable compared to fusion due to shorter operating time, faster patient recoveries, less blood loss, less narcotic usage, and shorter hospital stays, all with more sustained clinical success. If you’re suffering from spinal stenosis and considering surgery, come see us at Prairie Spine where the best options are made available to you.
About The Author: Derek N. Morrow, PA-C is a physician assistant with Prairie Spine and Pain Institute. Derek works in the clinic setting as a health care provider seeing patients. He is also utilized in the operating room as a first assist in surgery. In the clinic setting, his key function is to diagnose new patients and conduct their initial treatment. He works directly with patients to establish customized treatment programs and to monitor their progress. He also conducts history and physical evaluations for many patients. He performs many office procedures including trigger point injections, large joint injections, and bursa injections, all with the help of ultrasound guidance. He is radiologically trained, and uses his knowledge of X-ray, Ultrasound, MRI, CT, and EMG-Nerve Conduction Studies to establish a diagnosis and determine the appropriate treatment. Derek is surgically trained and plays a vital role in the procedures we perform at Prairie Spine and Pain Institute.