 If I have a back condition, why do I have leg pain?
If I have a back condition, why do I have leg pain?
This is a common question encountered in the spine world.
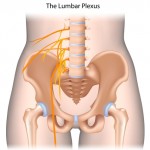
Lumbar radiculopathy is a disease process that affects one or more lumbar nerve roots. The lumbar spine consists of five vertebral moveable bones (block–like structures). The bones are labeled by number L-1, L-2, L-3, etc. In between each of the vertebral bones are shock absorbers, or what we call discs. Directly below each vertebral bone there is a pair of neural foramen, a hole-like structure for nerves to exit the spinal cord and move down the legs. Imagine tree roots (nerve roots) leaving the tree trunk (spinal cord); the holes (neural foramen) are located on the sides and just below the vertebral bodies. They are extremely important because a nerve lies inside each neural foramen.
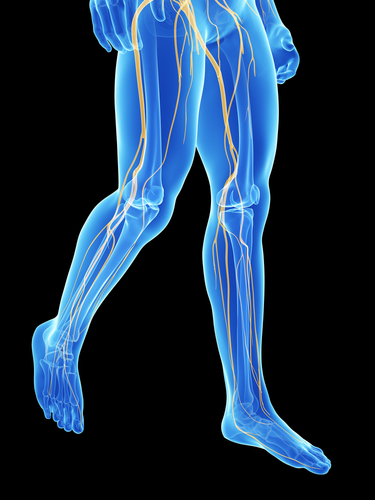
The nerves are labeled much like the vertebral bodies (L1 nerve root, L2 nerve root, etc). When something invades this neural foramen, a nerve can be compressed. This phenomenon is the magic and the spine patient’s dreaded symptom of lumbar radiculopathy. Lumbar nerve roots exit the spinal cord in the lower back, and travel all the way down the legs and into the feet—depending on which nerve root it is.
So, let’s recap!
Why do I have leg pain when the problem is in my back? Yes, the nerve root is compressed in the back, but the path of the nerves runs all the way down the legs in specific patterns. This process can produce shooting pains, numbness, tingling, and sometimes even muscle cramping in those specific patterns, thus = radiculopathy.
 Radiculopathy can be diagnosed clinically based on symptoms and physical exam findings. However, certain testing is sometimes required to confirm the diagnosis, such as an MRI or EMG Nerve Conduction Study. Once the diagnosis is made, treatment can then be focused on the specific affected nerve root. Treatment is often initiated in a conservative manner, generally in the form of physical therapy, medications, and possibly injections. The goal of any form of treatment should be to give the patient the most relief with the least amount of risk possible. (Translation: avoid being cut open for surgery if you can fix your back in a non-operative manner.)
Radiculopathy can be diagnosed clinically based on symptoms and physical exam findings. However, certain testing is sometimes required to confirm the diagnosis, such as an MRI or EMG Nerve Conduction Study. Once the diagnosis is made, treatment can then be focused on the specific affected nerve root. Treatment is often initiated in a conservative manner, generally in the form of physical therapy, medications, and possibly injections. The goal of any form of treatment should be to give the patient the most relief with the least amount of risk possible. (Translation: avoid being cut open for surgery if you can fix your back in a non-operative manner.)
When large injuries occur and the damage is significant, certain patients are pushed to the operating room more quickly than the average patient. Additionally, a patient with a resistant condition to conservative treatment might also make it to the operating room. In summary, being diagnosed with lumbar radiculopathy is a fancy way of saying you have a nerve root being compressed in the lower back that is causing radiating–type pain down the legs. If you are suffering from the aforementioned symptoms, come see us at Prairie Spine & Pain Institute so we can educate you more about your condition and get you started on a path to pain relief and functional improvement!
About The Author: Derek N. Morrow, PA-C is a physician assistant with Prairie Spine and Pain Institute. Derek works in the clinic setting as a health care provider seeing patients. He is also utilized in the operating room as a first assist in surgery. In the clinic setting, his key function is to diagnose new patients and conduct their initial treatment. He works directly with patients to establish customized treatment programs and to monitor their progress. He also conducts history and physical evaluations for many patients. He performs many office procedures including trigger point injections, large joint injections, and bursa injections, all with the help of ultrasound guidance. He is radiologically trained, and uses his knowledge of X-ray, Ultrasound, MRI, CT, and EMG-Nerve Conduction Studies to establish a diagnosis and determine the appropriate treatment. Derek is surgically trained and plays a vital role in the procedures we perform at Prairie Spine and Pain Institute.