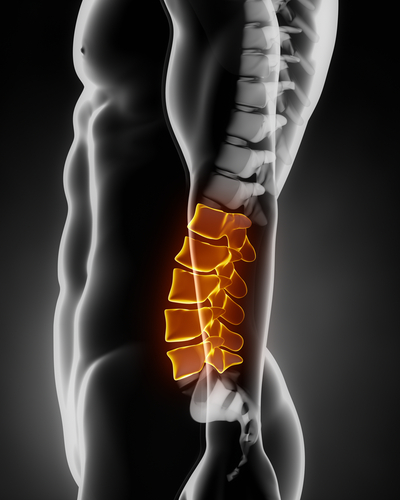
 In the lumbar spine, there are five vertebrae or bones separated by five intervertebral discs.
In the lumbar spine, there are five vertebrae or bones separated by five intervertebral discs.
The lumbar vertebrae are named one through five with lumbar vertebral body one being the superior most and lumbar five being the inferior most. The disc spaces in between are named by the vertebrae above and below, for example L3-L4 disc. There are two main disc functions. The first is to act as a shock absorber for the spine. These cushion like structures help when there is axial loading, or when a person is standing upright increasing the pressure on the disk. The other function is to hold the vertebrae above and below together while allowing slight movements. The movements are demonstrated by the ability to bend forward, backward, side to side, and rotate left or right. Without the discs there would be no range of motion of the spine.
 When trying to find the pain generator in a person with low back pain, it is important to always keep in mind the discs as a potential source. Typically, discogenic pain is exacerbated with increase in axial loading or increase in disc pressure. Patients are most vulnerable when they are sitting/standing, bending forward, coughing or sneezing. These types of movements can increase disk pressure and provoke the disc pain. The reason pain is felt is due to the innervation of nerves on the outer portion of the disc called the annulus fibrosus. The inside of the disc (nucleus pulposus) does not have a nerve supply. However when there is disruption in the central portion of the disc substances can leak out into the anular portion of the disc causing discogenic pain. Discs, like many other things in the body go through wear and tear processes overtime and eventually can break down. This concept is similar to arthritic changes in major joints such as knees being bone on bone. When discogenic pain is suspected often further diagnostic testing is needed.
When trying to find the pain generator in a person with low back pain, it is important to always keep in mind the discs as a potential source. Typically, discogenic pain is exacerbated with increase in axial loading or increase in disc pressure. Patients are most vulnerable when they are sitting/standing, bending forward, coughing or sneezing. These types of movements can increase disk pressure and provoke the disc pain. The reason pain is felt is due to the innervation of nerves on the outer portion of the disc called the annulus fibrosus. The inside of the disc (nucleus pulposus) does not have a nerve supply. However when there is disruption in the central portion of the disc substances can leak out into the anular portion of the disc causing discogenic pain. Discs, like many other things in the body go through wear and tear processes overtime and eventually can break down. This concept is similar to arthritic changes in major joints such as knees being bone on bone. When discogenic pain is suspected often further diagnostic testing is needed.
One tool often utilized in spine orthopaedics is provocative discograms. When there is suspicion that a disc could be causing the majority of a patient’s low back pain, discograms are often performed. Needles are inserted into a pressurized disc, and contrast dye is injected into the discs to see if the same pain is provoked that the patient has at home. To be positive, it is imperitive the pain be exactly the pain a patient experiences when he or she is at home, and the pain should increase as the dye increases in the disc pressure.
About The Author: Derek N. Morrow, PA-C is a physician assistant with Prairie Spine and Pain Institute. Derek works in the clinic setting as a health care provider seeing patients. He is also utilized in the operating room as a first assist in surgery. In the clinic setting, his key function is to diagnose new patients and conduct their initial treatment. He works directly with patients to establish customized treatment programs and to monitor their progress. He also conducts history and physical evaluations for many patients. He performs many office procedures including trigger point injections, large joint injections, and bursa injections, all with the help of ultrasound guidance. He is radiologically trained, and uses his knowledge of X-ray, Ultrasound, MRI, CT, and EMG-Nerve Conduction Studies to establish a diagnosis and determine the appropriate treatment. Derek is surgically trained and plays a vital role in the procedures we perform at Prairie Spine and Pain Institute.